PREVIOUS: MBTI Basics #2a
PREVIOUS: MBTI Basics #2a
OVERVIEW of MBTI dichotomies (cont.)
The 2 ‘INNER’ (S-iN & T-F)
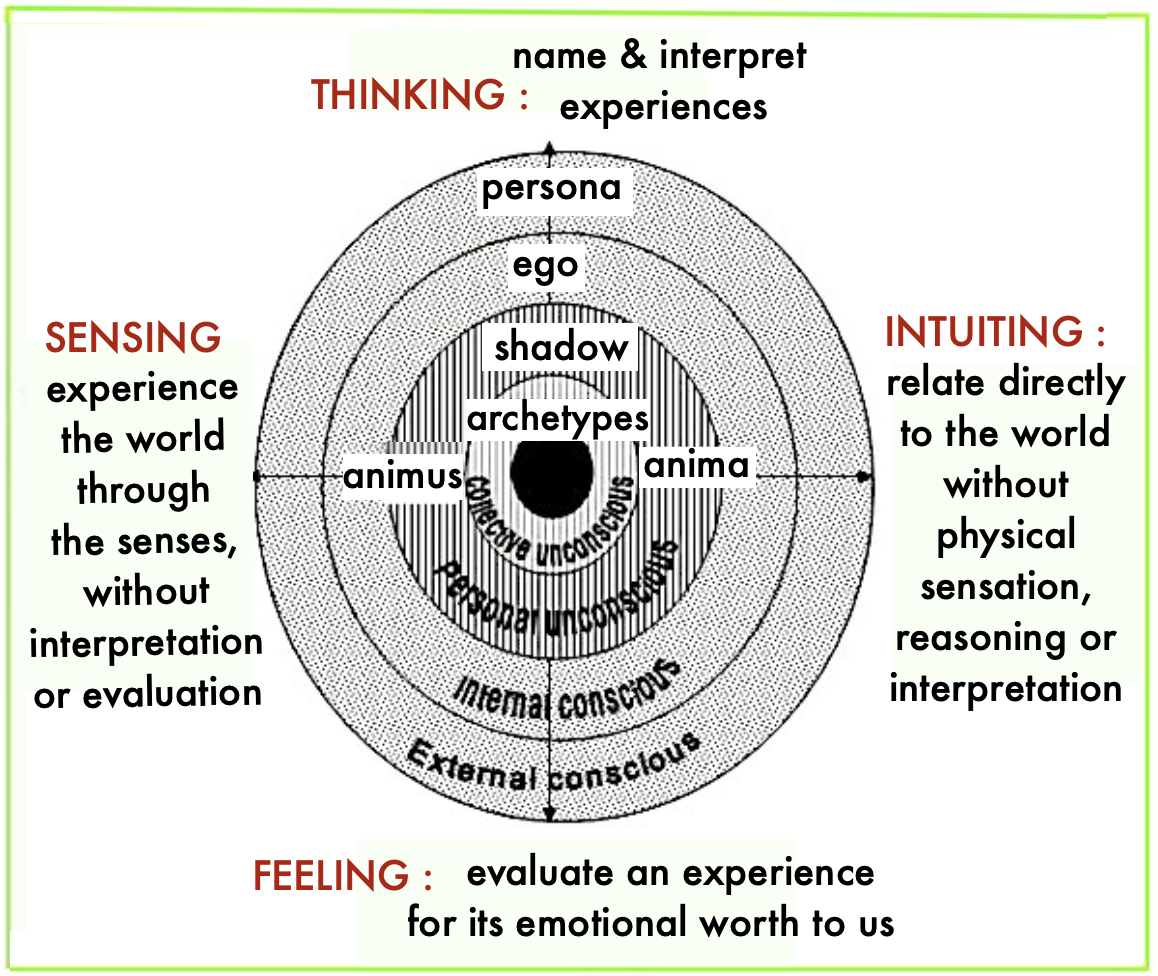
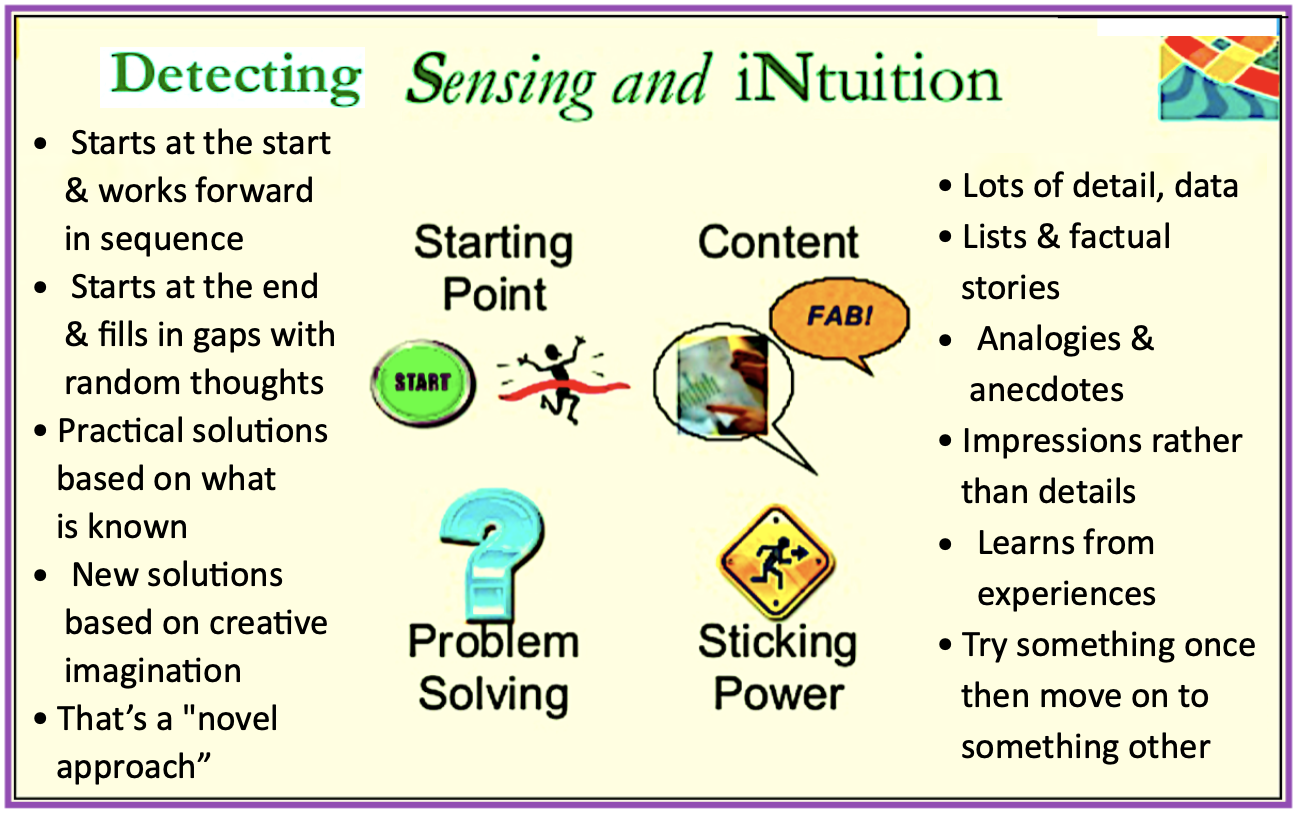
2. SENSING (S) vs INTUITION (iN)
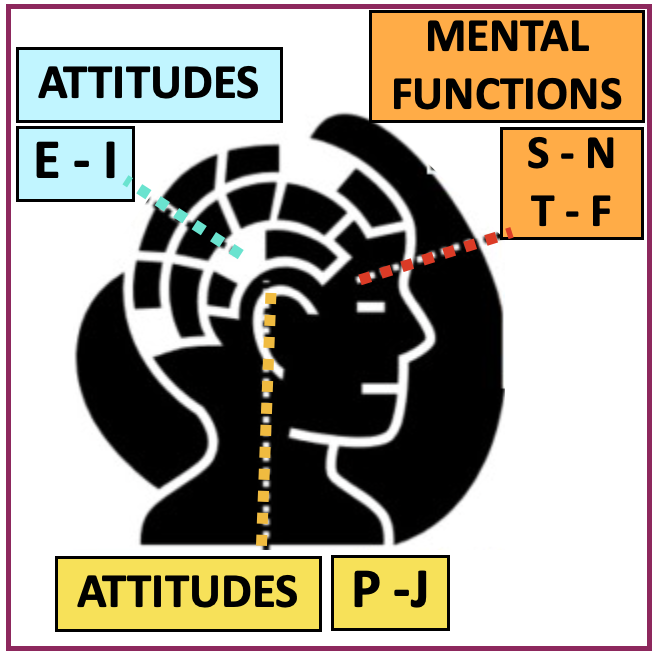
The kind of INFORMATION we prefer to gather & trust. It can be either Introverted or Extroverted (Si or Se / iNi or iNe) , & each part of the Judging style. We use both, but to different degrees of effectiveness & with different levels of comfort. 
• Sensing (S) / Concrete
To be mainly Sensate means that a person primarily believes in the kind of information he/she receives directly from the external world.
They absorb info thru the 5 senses – are detail oriented (micro) types, who prefer to focus on facts & concrete data, wanting to see the hard numbers.
They keep track of available material & resources, appreciate knowing the “HOW” of something, & then do what works. They love to observe, are good at remembering specifics, & understand things piecemeal, working through concepts from the bottom up.
Sensors LOOK for: how much, how many, how often, what kind….
EXP: When we – taste food / notice a stoplight has changed / memorize a speech / follow steps in a plan / use a map / look up info on Google….
— 🍀 —
• Intuition (N) /Abstract
To be mainly Intuitive means that a person more likely believes the kind of information they  gather from their internal, private world.
gather from their internal, private world.
They’re are highly imaginative, focusing on patterns & the meaning of data, taking in info from impressions, insights & patterns. They start with the big-picture (macro), extrapolating abstract possibilities from a wide variety of ‘real’ sources, understanding concepts using a top-down approach, & data as it relates to other data. They have a grasp on trends, interested in what hasn’t been tried before.
Intuiters ASK: “….for example? / Tell me more, what else should I know? /Why do you say that? “-…. and then echo the response
 EXP: Those who find a new way of doing something / think about future implications for a current action / ‘get’ the underlying meaning in what people say or do / see the big picture….
EXP: Those who find a new way of doing something / think about future implications for a current action / ‘get’ the underlying meaning in what people say or do / see the big picture….
NOTE: Of the 4 dichotomies, at their extremes these 2 opposites cause the most emotional difficulty in any relationship. Such people tend to be highly frustrated by & may even feel disdain for each other’s style. It can be particularly painful for a sensitive child -strongly NF- to be raised by a mother who is strongly ST.
✓ Ns use the same concrete / real-world experiences to ‘see’ things as Ss, but much of it is subliminal, so they can’t always put into words how they reached conclusions – they just know.
✓ To the S this is hocus-pocus, since they don’t trust anything they don’t gather from their own experience or from empirical research, & which can be clearly, logically verbalized. 3. THINKING (T) vs FEELING (F)
3. THINKING (T) vs FEELING (F)
Preferred way of coming to DECISIONS. Can be either Introverted or Extroverted (Ti or Te / Fi or Fe) , & each is part of the Perceiving style
We all use both forms, but put more trust in one, some decisions being made entirely from the T or the F s ide.
ide.
What makes some Decisions very difficult is when there’s an intense conflict between head & heart (T & F), in which case our dominant preference will win.
Easier decisions, the ones that feel good, are usually the result of our T & F sides being ‘on the same page’ (in agreement).
• Thinking (T) – These are the analytical/ logic types – but does not indicate how smart one is. They tend to make decisions in a rational, impartial way, based on what they  believe to be correct info, using pre-defined axioms & rules of behavior, as well as Fairness (everyone treated equally).
believe to be correct info, using pre-defined axioms & rules of behavior, as well as Fairness (everyone treated equally).
Ts assess & analyze whether the info received makes sense & whether or not something works – such as the concept of gravity. Then decisions come from using cause/effect, if/then, true/false choices to for validity.
EXP: Those who research a product via Consumer Reports, buy the best one to meet their needs, whether or not they like it, do the ‘Right Thing’, form guidelines to follow for performing tasks …. (Re. HATS ➡️ )
— 💛 —
 • Feeling (F) – The importance of info is determine holistically, & perceptions are evaluated based on a sense of harmony, to maintain peace. It’s about making value judgements – whether things are good or bad.
• Feeling (F) – The importance of info is determine holistically, & perceptions are evaluated based on a sense of harmony, to maintain peace. It’s about making value judgements – whether things are good or bad.
EXP: The person who ‘Feels’ that stealing is right/wrong
NOTE: This MBTI category is not about emotion, but rather a reasoning process handled in the higher brain (cortex). Contrast this with the inner brain’s limbic system which responds to stimuli we (call) experience as emotion.
‘Feelers’ are more empathic (pick up on others’ emotions), make subjective decisions on a case-by-case basis, & use feelings they believe to be right rooted in their own values. Here ‘Fairness’ means that individuals is treated equally.
 EXP: When we – buy something because we like it / don’t say something that ‘ll upset another person / decide not to take a job because we don’t like the work environment / decide to move somewhere new to be close to someone we care about….
EXP: When we – buy something because we like it / don’t say something that ‘ll upset another person / decide not to take a job because we don’t like the work environment / decide to move somewhere new to be close to someone we care about….
NOTE: The Thinking – Feeling level is the only one that generates a gender bias.
The Thinking Woman swims against the current in most areas of life, especially at work. If she’s decisive & objective — she’s branded hard, cold, unfeminine……
The Feeling Male is also disrespected – called soft, weak, a pushover …… for having a caring nature.
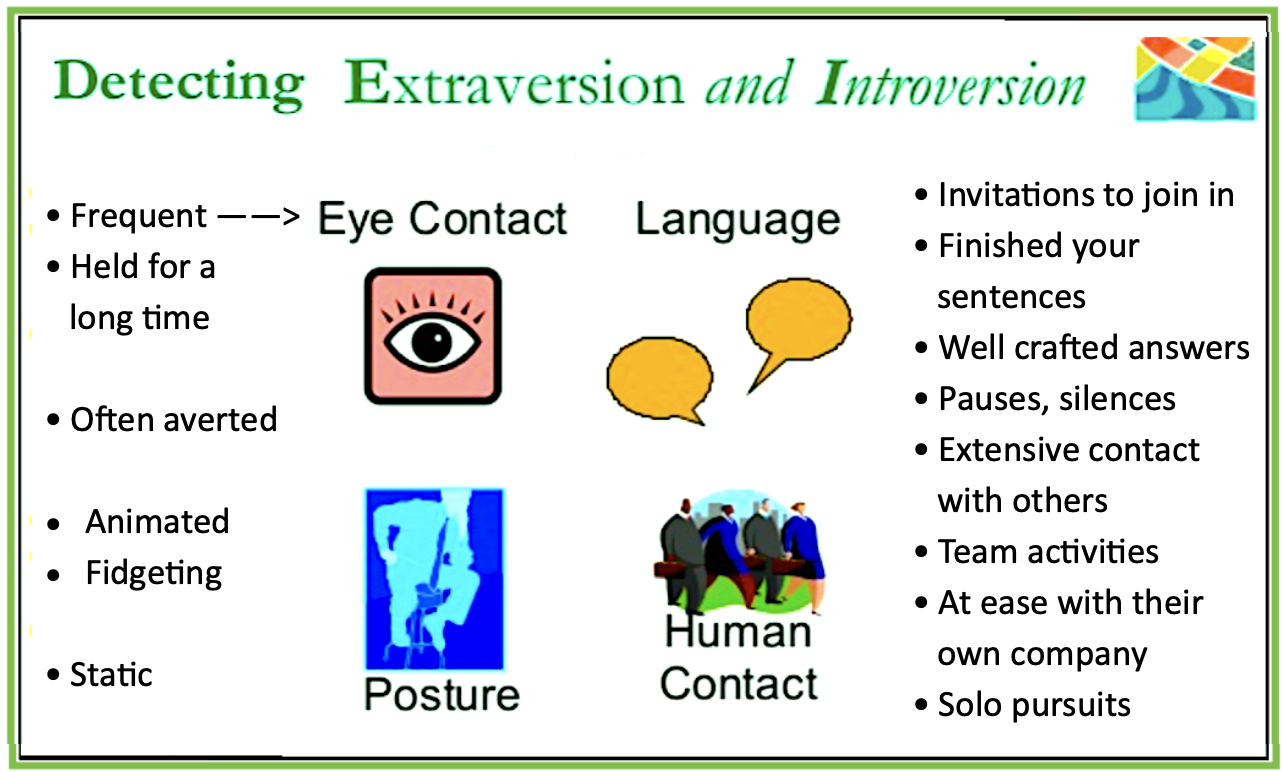
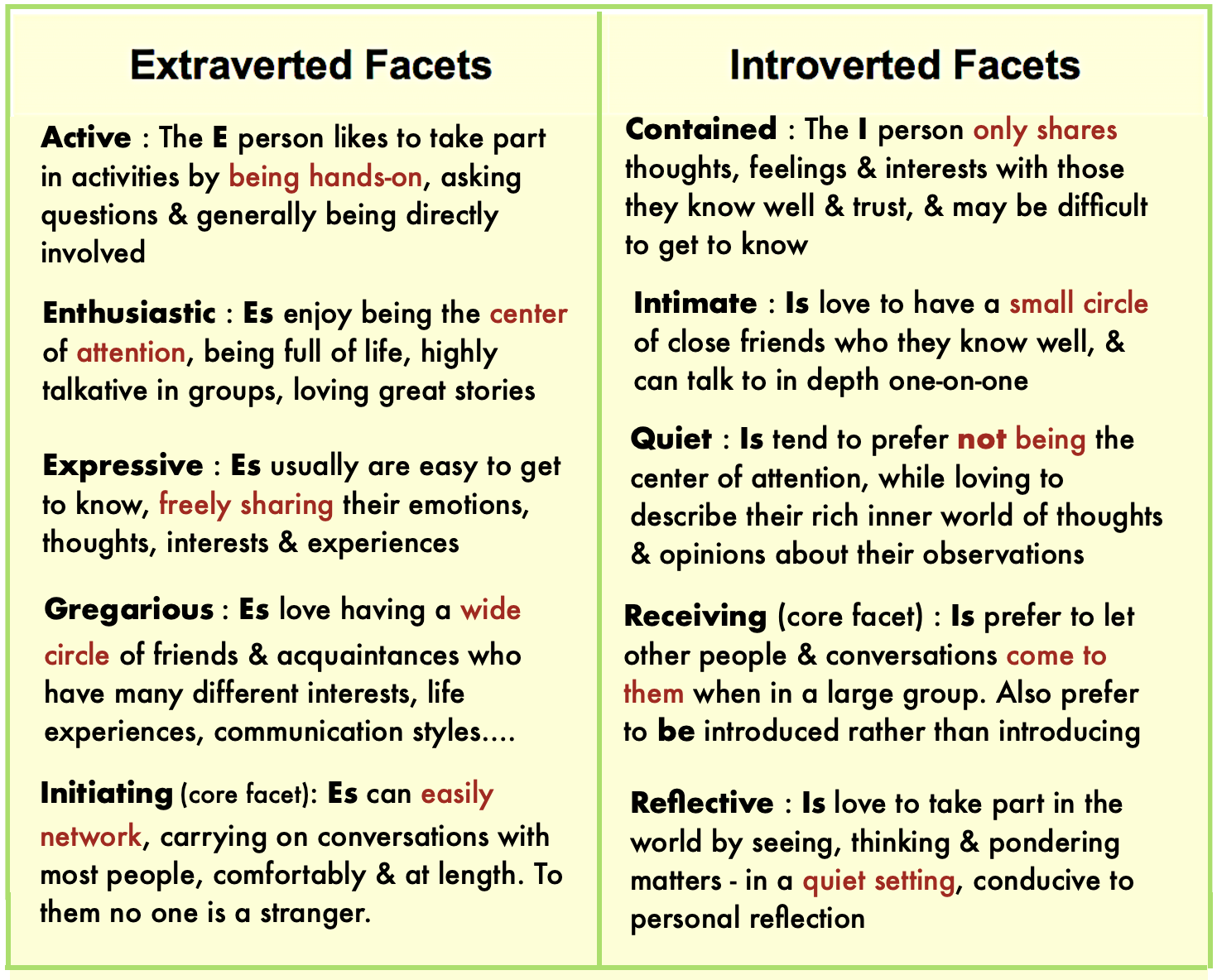
NEXT: Intro- Extra-verts
Share this: LinkedIn, Reddit, Pinterest

 PREVIOUS:
PREVIOUS:
 Beside the basic MBTI designation (INTP….), each type has a <—- ‘Cognitive Function stack, & a Temperament (Artisan, Guardian….) in combinations of the basic 8 options (NT, SJ….). Along with the MBTI, each of us also has our own Enneagram Type, Astrology sign, childhood experiences, social environment.spiritual belief,…. & taken together they make up our identity.
Beside the basic MBTI designation (INTP….), each type has a <—- ‘Cognitive Function stack, & a Temperament (Artisan, Guardian….) in combinations of the basic 8 options (NT, SJ….). Along with the MBTI, each of us also has our own Enneagram Type, Astrology sign, childhood experiences, social environment.spiritual belief,…. & taken together they make up our identity.























 I
I