PREVIOUS : Attachment & FOOD (#4a
PREVIOUS : Attachment & FOOD (#4a
IMAGE ⬆️ = Regions w/ associated behaviors & functions
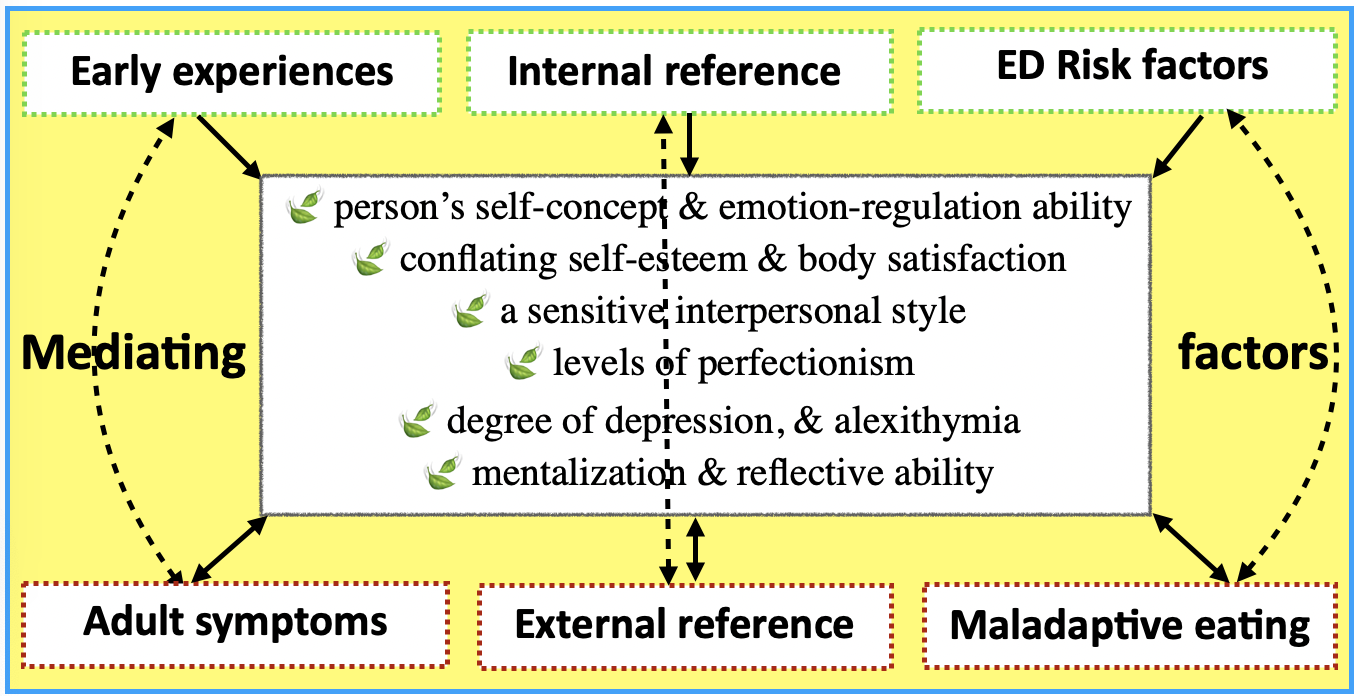
SITE : Attachment Theory in the Treatment of Bulimia
CNS Regulation of Binge- & Over- Eating
RESEARCH : Appetite & body weight regulation are controlled by the body’s central nervous system (CNS), the brain playing a central role in integrating inner & outer inputs to keep energy provisions in balance. Circuitry which controls eating is regulated by the attention, emotion/memory, cognitive-control & reward systems.
Changes in mental & emotional processes are implicated in the dysregulation of human eating behavior. Techniques used to examine appetitive include neuro-cognitive testing (via computer games), fMRI, PET & SPECT scans. Together they revealed the neuro-chemical determinants critical to understanding how the reward center in the brain is altered in obesity & emotional eating. Brain LOBES ➡️
Some RESULTS
Insecure Attachment & their subtypes are linked to many brain functions : 13 executive regions, 6 affect (emotions), 6 reward, 3 sensory, 1 social & 1 cerebellar.
CHANGEs found in the :
— Executive function = high frequency of externalizing behaviors (aggression, antisocial & behavioral problems)
— Affective processing = high frequency of internalizing behavioral disorders (anxiety, depression, suicidality)
— Reward regions = higher frequency of substance abuse
— Social circuits = high frequency of excessive help-seeking, dependency & excessive social isolation
Insecure adults required more of their executive control functions when faced with attachment-relevant stimuli (listen to infant crying) – staying in the head to not feel. The excess stress could relate to a high prevalence of personality disorders.
— Resistant types, being highly emotional & obsessive, were less able to gather brain resources to stop negative thoughts
— Avoidants showed poorer memory of attachment-related events (childhood trauma), linked to a higher prevalence of conduct disorders.
♦︎ ♦︎ ♦︎
BULIMIA
 The term refers to an eating disorder (ED) characterized by episodes of binge eating followed by compensatory behaviors such as purging, fasting, and/or excessive exercise.. It is the result of genetic predisposition along with the influence of psychosocial &/or environmental triggers.
The term refers to an eating disorder (ED) characterized by episodes of binge eating followed by compensatory behaviors such as purging, fasting, and/or excessive exercise.. It is the result of genetic predisposition along with the influence of psychosocial &/or environmental triggers.
Many studies have proven overlapping behaviors & addictive personality traits of substance abusers & Bulimics. In fact this ED commonly co-occurs with drug addictions,
EXP: the National Center on Addiction & Substance Abuse has shown that approximately 35% of all alcoholic women also have an ED. And 50% of people with EDs also struggle with substance abuse.
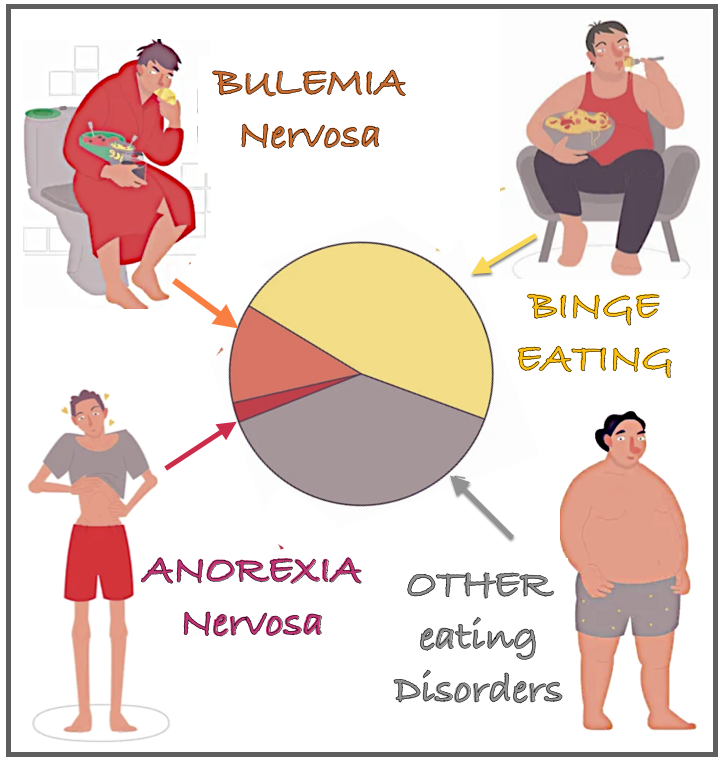
2 TYPES – Because symptoms & behaviors of Bulimia are complex, it’s divided into :
Purging – The most commonly understood version, which involves the person binge eating, followed by such behaviors as vomiting &/or laxative/ diuretics/ enemas.
Non-Purging – This group do not expel food from the body as a way to deal with their self-loathing. Instead, they compensate by fasting or compulsive exercise, & rarely if ever purge.
A faulty reward-processing system seems to be an important feature of the diseases.
Brain studies reveal that neurological abnormalities contribute to the development of bulimia, a result of altered brain chemicals such as serotonin levels, which contribute to the dysregulation of mood, appetite, & impulse control.
EXP : Dopamine activity is altered in both bulimia & anorexia — but in opposite ways. While the reward circuits in women with anorexia are overly sensitive to food-related stimuli, women with Bulimia have a weaker-than-normal response in brain regions that are part of the dopamine-related reward circuitry.
 STATISTICS = In the US as of 2023, Bulimia Nervosa :
STATISTICS = In the US as of 2023, Bulimia Nervosa :
▶︎ affects 4.7 million women, & 1.5 million men, although the number of males being diagnosed is expected to increase because of better awareness of how males display symptoms.
 ▶︎ As much as 25% of college age females use bingeing & purging as a weight loss method , with an average onset age of 18. Overall –
▶︎ As much as 25% of college age females use bingeing & purging as a weight loss method , with an average onset age of 18. Overall –
▶︎ 78% experience daily life impairment
▶︎ 43.9% experience severe impairment
▶︎ 8% are female, lasting more than 5 years, 5x more the men
▶︎ Only 3% receive treatment
▶︎ 3.9% will die from the disorder.
Bulimics are more likely to come from a family with a history of eating disorders, physical illness, & other mental health problems. Adult traits include the tendency to impulsivity & sensation seeking, typically present from childhood. But they have a secret life, keeping their eating disorder very private & hidden.
«
«
NEXT : Attachment, Food & Others, #4c