PREVIOUS : Attachment & Animals #6
PREVIOUS : Attachment & Animals #6
SITE :
Sex & Intimacy (many articles)
“Attachment & sexuality impinge on and influence each other. This occurs in other species as well as for humans”. Bowlby (1969)
Gurit E. Birnbaum, Ph.D. : “Sex does not exist in a vacuum. Rather, sexual functioning is likely influenced by views of self & others developed out of early attachment experiences with primary caregivers.
The person’s chosen style (Secure, Anxious, Avoidant) guide their interpersonal interactions over an entire life, which is likely to affect the functioning of their later-maturing sexuality : why people engage in sex, what do they seek from their partners, & how they get their needs met – if at all.
Each of these strategies is driven by specific anxiety, & is intended to ‘satisfy’ interpersonal goals that help cope with these fears.
Emory neuro-scientist Thomas R. Insel wrote :”Virtually every form of psycho-pathology is characterized by abnormal social attachments.”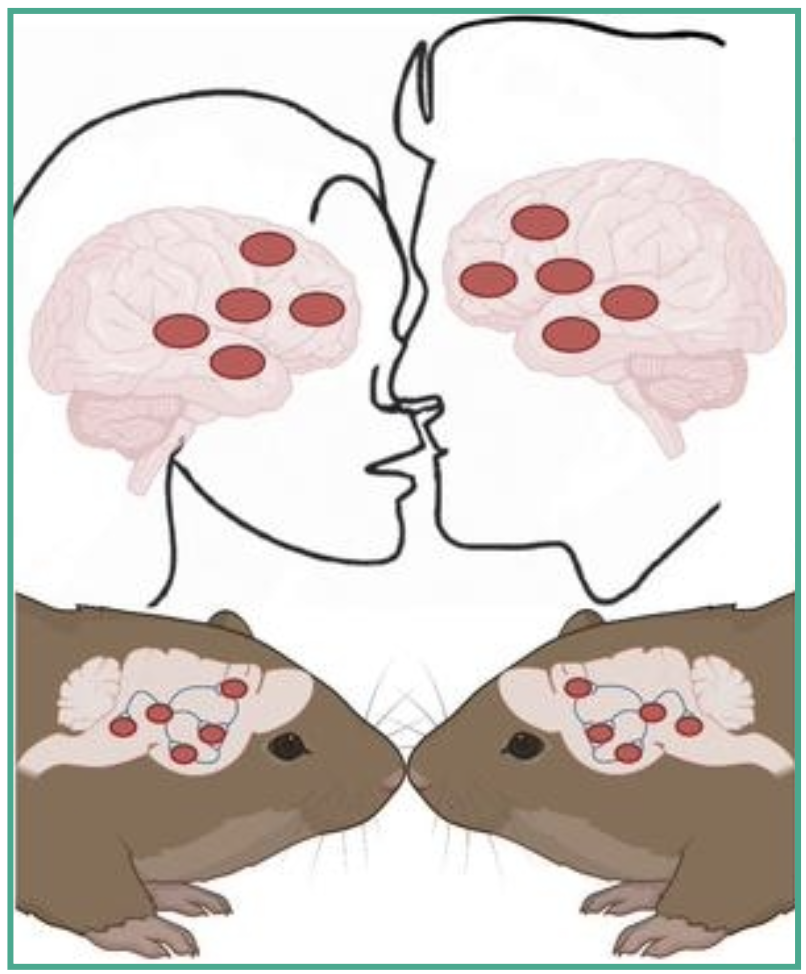
For 15 years Insel has been studying highly social prairie voles, & found they are a model of ‘family values’. They naturally form lasting, monogamous male-female pair bonds, & prefer the company of their mate over others.
❇️ These characteristics can be attributed to the peptide hormones oxytocin (OT) in females, & vasopressin (AVP), in males. Insel :”Apparently, at least in voles, these 2 systems are activated by pair bonding.”
Insel & his team’s research is not on a hunt for fairy love dust or an elixir for fidelity. Instead, they want to find answers to the more pressing problems of millions of people with severe mental illness, who are not able to form normal social bonds, robbing them of the very fundamentals of human interaction & communication.
re. ATTACHMENT : “Across human cultures, sexual behavior is consistently associated with pair bonding, although sex is neither necessary nor sufficient for bond-formation.”
⬆️ An interesting combination of brain chemicals : In human males, AVP (m) peaks during arousal, & oxytocin (f) peaks with ejaculation. (More….)
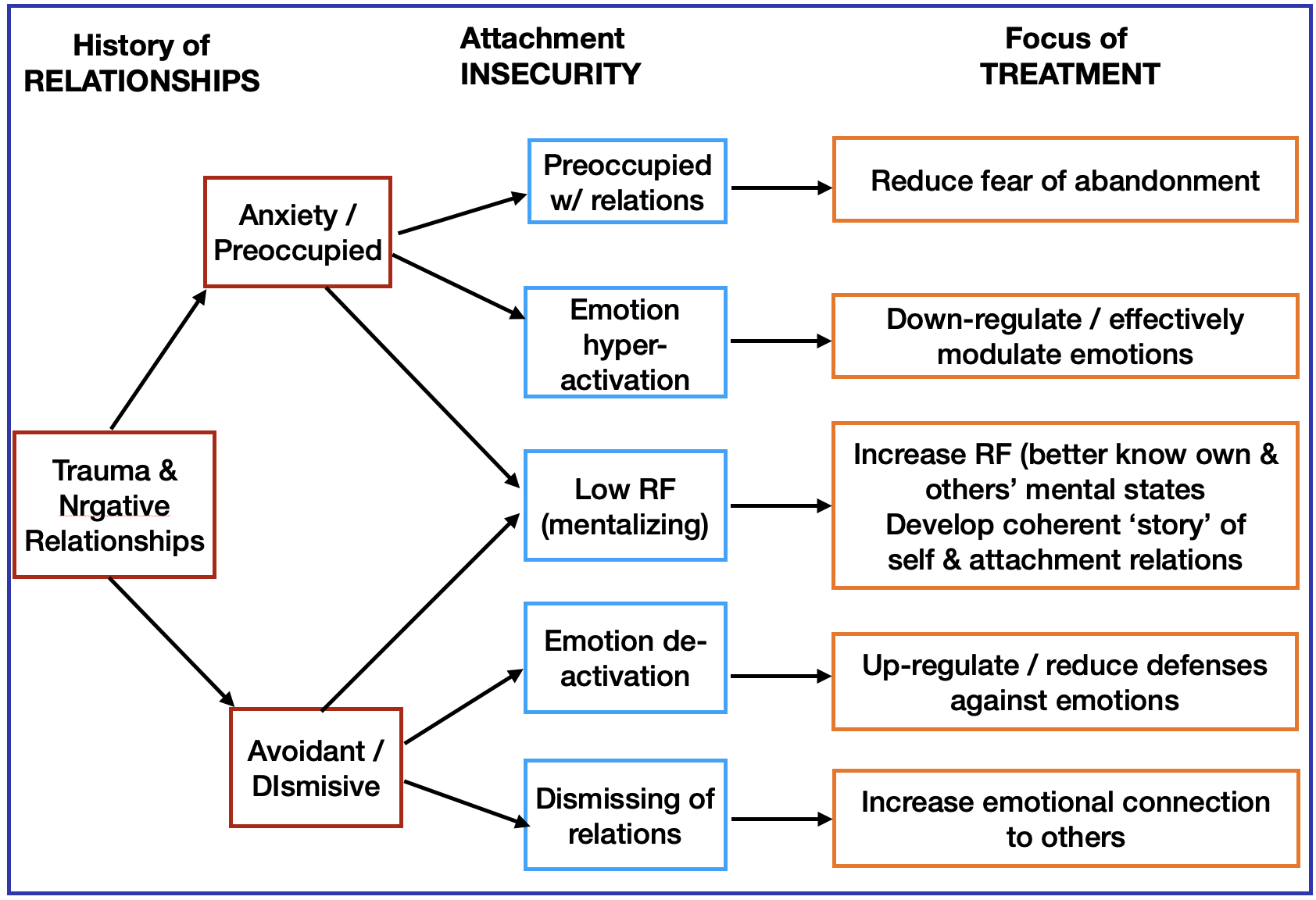
2 INSECURE Styles
While as human beings, we can indeed separate love and sex, they are designed to be together. In “Love Sense”, by Dr. Johnson :
 1. Sex without love is defined as “sealed off sex”. When sex is detached from a sense of connection with a partner, it increases their desire to experience new partners & new ways to have sex. A a sexual abuse history or porn addiction (or both) are common causes for a person to disconnect their emotions from adult sexual activity.
1. Sex without love is defined as “sealed off sex”. When sex is detached from a sense of connection with a partner, it increases their desire to experience new partners & new ways to have sex. A a sexual abuse history or porn addiction (or both) are common causes for a person to disconnect their emotions from adult sexual activity.
Not surprisingly, sealed-off-sex can lead to relationship troubles, because the connection between partners is lost, & resentment brews. As the distance widens, it can cause fights, abusive communicating, & infidelity, when one or both people get pulled into another relationship to compensate for what/s lacking in their current one.
2. Dr. Johnson also identified “solace sex” . If one or both partners doubt their mate’s love & caring for them, AND they’re afraid of their own emotional needs & too anxious to openly tell their partner —-> they start using sex as a way to soothe their fears.
In this case, couples may have sex frequently, instigated by the more insecure one – as a demand for sex many times a day or a week – to be reassured of their partner’s love. It’s as if they’re saying, “I’m unsure you love me, so I need you to ‘show’ me with frequent & intense sex.”
But it’s never satisfying or healing, because by itself it doesn’t develop self-esteem, so they can’t be emotionally vulnerable or trust that the partner genuinely cares.
Relationship problems can include resentment building up in the partner who is being pressured to perform, which increases the insecurity in the one looking to find solace through sex.
SITE: : A positive view of Solace Sex
 Loving sexual passion can help heal insecure emotional attachment.
Loving sexual passion can help heal insecure emotional attachment.
◆ For anxiously attached WOMEN — sexual desire from their partner is deeply reassuring & emotionally stabilizing, allowing them to fall in love & be loved
◆ For anxiously attached MEN, sex creates a positive effect on the relationship soon after the sexual encounter.
For avoidant males, when their sexual desire-cues are responded to positively – it gives them the feeling that this relationship might be sexually & emotionally safe, so they can open up more.
NEXT : Sexuality INTRO, #2