PREVIOUS : Attachment & SEXUALITY – INTRO (#1)
PREVIOUS : Attachment & SEXUALITY – INTRO (#1)
SITE : “Here’s what happens to the body during sex” – very interesting
PURPOSE
While we may think our reasons for having sex are unique to the moment, we can identify our MOTIVES into 4 categories:
1. Intimacy : the desire to feel connected & express love
2. Pleasure : to enjoy our bodies in relationship with our partner’s body
3. Approval : to prove attractiveness, find reassurance, avoid conflict, please partner
4. Coping : minimize unpleasant emotions, self-soothe, gain a sense of status or power
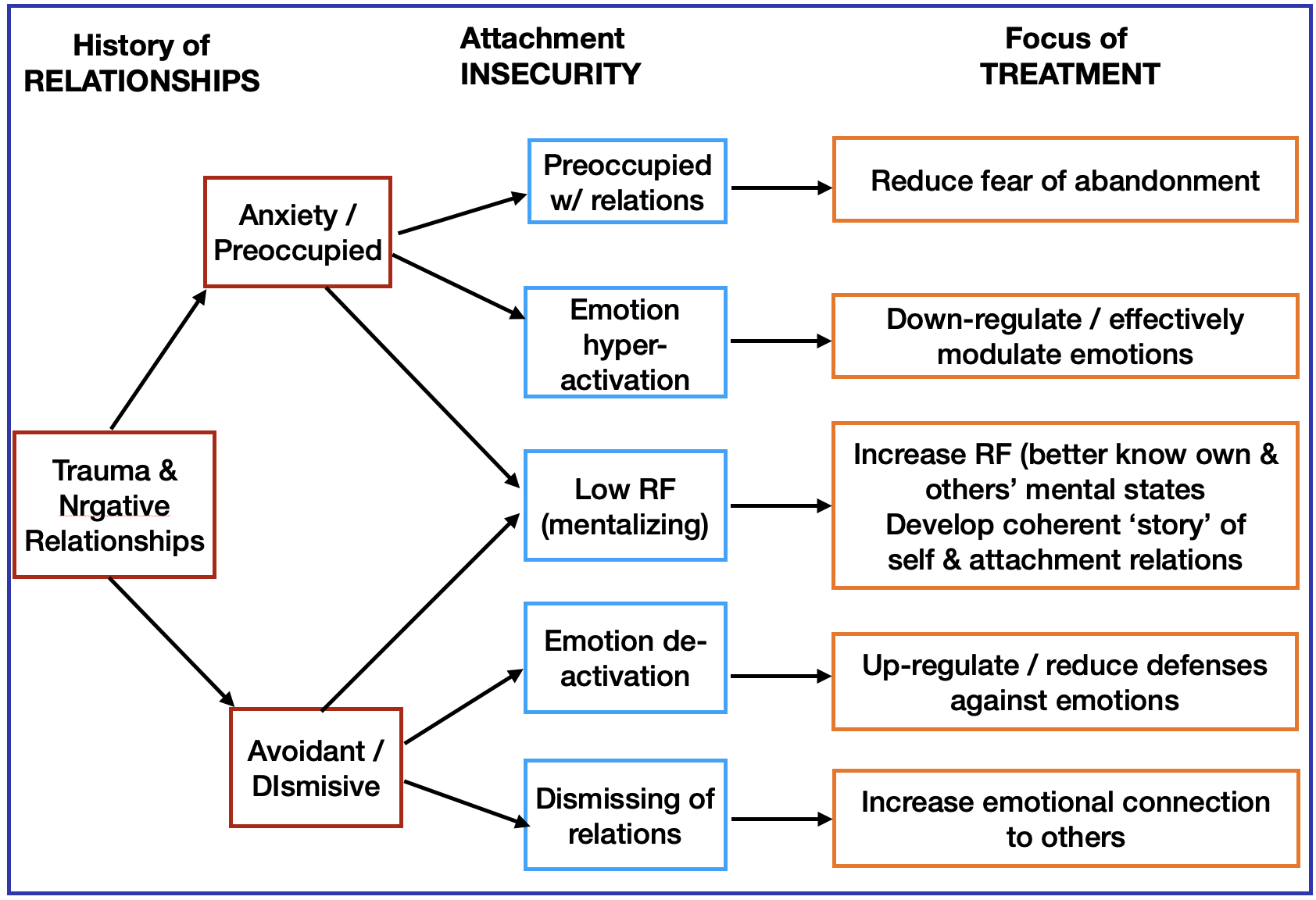
Emotional Attachment styles interacting with Sexual Behavior
Motives 1 & 2: Securely attached couples have 2 main sexual motives: intimacy and pleasure + a strong commitment to each other. When in love, the secure emotional connection makes it easier for the couple to be present, authentic & vulnerable. Initiating sex is more mutual.
Delight in touching, enjoyment of sexual variety, & a desire for genital pleasure — brings tremendous physical excitement. This adds more satisfaction & intimacy to their sexual experience.
Motives 3 & 1: An Anxiously attached partner’s motives are more about approval – mainly to eliminate feeling inadequate & unattractive, as well as to ‘generate’ love, & from obsession with their romantic partner. Yet, they may prefer the show of affection during sex, being less motivated by pleasure, or even uncomfortable with direct genital stimulation.
 Unfortunately, because of their own concern for reassurance & safety (which sex can help with!) they’e less attuned to their partner’s sexual needs & preferences, being more worried about their partner’s love, and their own performance.
Unfortunately, because of their own concern for reassurance & safety (which sex can help with!) they’e less attuned to their partner’s sexual needs & preferences, being more worried about their partner’s love, and their own performance.
In their insecurity, they can miss the chance to shape the sexual experience in ways that are sexually exciting for themself. This can lead to low desire, being disconnected from the pleasure motive (Point 2).
 Motives 4 & 2: Avoidantly attached partners often have sex trying to manage the internal stress of negative feelings such as fear, sadness, emptiness…. & for pleasure too, but mainly without commitment. They’re more likely to have casual sex, be unfaithful, or use sexual conquests to prove their power.
Motives 4 & 2: Avoidantly attached partners often have sex trying to manage the internal stress of negative feelings such as fear, sadness, emptiness…. & for pleasure too, but mainly without commitment. They’re more likely to have casual sex, be unfaithful, or use sexual conquests to prove their power.
They compartmentalize pleasure away from intimacy, finding the emotionally intimate past of the sexual encounter hard to face. To stay self-reliant when in a committed partnership, some Avoidants will prefer to masturbate rather than negotiate with their partner for sex, likely disappointing & frustrating the mate.
EXP : when one partner habitually uses sex as a “sleeping pill’ to cope with stress, the other one won’t feel loved or excited by sexual requests when they do occur. Or, maybe the ‘waiting’ partner is the type to acquiesce, but just wants to get it over with quickly, so doesn’t mind sexual advances being rare.
PROMISCUITY = a complex combination of ‘short-term mating’ with multiple partners during a person’s life, without any of the relationships being exclusive or monogamous . Whether this behavior is acceptable or not is considered a matter of personal opinion. 
What motivates someone to be promiscuous varies.
♦︎ Attachment Theory says that people who had a poor relationship with parents in childhood are more likely to become promiscuous as adults, used as temporary relief from the anxiety associated with having an Insecure attachment.
In contrast, people with an original Secure attachment developed with parents, are less motivated to ‘stray’. However, some theorists believe that one’s gender is a main factor in promiscuity. The Sexual Strategies Theory argues this is because males – tend to prefer short-term relationships, agree to have sex sooner than females, & have a desire for multiple sex partners.
♦︎ According to the Drive Reduction Theory – to engage in sexual behavior in the first place – the person must feel some level of physical deprivation. However, it doesn’t imply that the need for sex is better met by short term mating.
 ♦︎ In addition, personality traits play a key role in promiscuity motivation. From the 5-Factor Theory, people high in Extraversion & low in Agreeableness / Conscientiousness are far more likely to have short-term encounters than those who are Introverted &/or high in Agreeableness/ Conscientiousness.
♦︎ In addition, personality traits play a key role in promiscuity motivation. From the 5-Factor Theory, people high in Extraversion & low in Agreeableness / Conscientiousness are far more likely to have short-term encounters than those who are Introverted &/or high in Agreeableness/ Conscientiousness.
➡️ It also seems that people who have a particularly warm (phlegmatic) or cold (melancholic) temperament are more likely to be promiscuous than moderate types. (More…. extensive info)
NEXT : Attachment & Sexuality